
.
Education Pleas
Millions of injured children whose pleas are not being heard are waiting at the intersection of the “Defending Childhood” Report from the U. S. Department of Justice (DOJ) and Congress’s rewrite of “No Child Left Behind” education (ESEA) legislation.
While the children wait for help, other education efforts are ineffective. Children and adults have the right to be frustrated and angry.
As one part of defending childhood, the children need pivotal changes when the adults in the House and Senate work to reconcile their differences on ESEA.

.
The children’s injuries are captured in a term from neurobiology: “childhood trauma”.
Childhood trauma is not “poverty”.
Sometimes ‘trauma’ and ‘poverty’ are misleadingly used interchangeably. Yet, research shows that more than half of those living in poverty do not experience debilitating trauma. Poverty does have a myriad of impacts on learning to be sure, but they are not necessarily traumatic impacts.
Childhood trauma is the response of overwhelming or helpless fear, or terror. Specifically, it is a response to abuse, neglect, to a missing parent, or a household which includes violence, mental illness, or substance abuse. Other childhood traumas can include experiences with community violence, or ethic oppression, and many more. Let’s be clear. Trauma means things like rape. Like physical beatings, like relentless emotional destruction, or maybe complete disregard for basic physical needs. Total neglect of another human being. Often the trauma is inflicted by someone who is a “caregiver”.
The magnitude is staggering! The DOJ Report described childhood exposure to violence and trauma as an “epidemic” back in 2012. Even earlier, back in 1979, the Surgeon General termed it a “national crisis”. In spite of the stunning scope, and life altering power, children are still being hurt today. To them it must seem like a never-ending nightmare!
We do know how to help.
Instead, at this particular intersection today, where children attempt to “achieve” in elementary and secondary school classrooms, the nightmare continues, and can often be worsened.
Congressional contact info is linked at the end of this blog, for those who are immediately ready to speak for the children.
.
Wide Scope: All Neighborhoods
Public health research by the CDC reveals devastation that is no respecter of demographics, zip code or socio-economic status. Specifically, researchers found that even in beautiful suburban San Diego, roughly one-fourth of the mostly middle class, mostly white, working folks with medical insurance had experienced 3 or more ACEs!
The wide scope varies in a shocking range from 22% to greater than 45% of children impacted by 3 or more categories of trauma — in many school districts the scope is greater than English Language Learners (ELL) or those with an Individual Education Plan (IEP). In some urban locations (pg. 17 map) the prevalence is greater than ELL and IEP students combined! Each of those impacts is acknowledged and accommodated and funded. Not childhood trauma.
Lifelong Impact
Three or more ACEs is significant because experiencing 3 or more ACEs correlates with doubled risk of depression, adolescent pregnancy, lung disease, and liver disease. It triples the risk of alcoholism and STDs. There is a 5X increase in attempted suicide. It doesn’t just go away. Later, if unaddressed, it results in work absenteeism and lost productivity, measured in billions of dollars. The CDC also found a “strong correlation between the extent of exposure to childhood ACEs and several leading causes of death in adulthood. . .”
.
Deep Impact: Life Changing
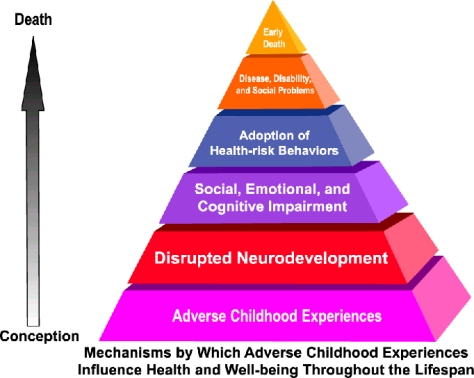
The deep impact of childhood trauma changes the architecture of children’s physical brains, and impairs their cognitive and social functioning.
Over time, trauma in childhood changes life trajectories and likely results in early death. See Levine and Kline p.4, Perry p.245, Perry (again), and the CDC Adverse Childhood Experience (ACE) research.
The neuroscience is compelling. Childhood trauma connects directly to education via its toxic stress effects on development of the physical brain. When children live in a chronic, traumatic state of survival, the unresolved toxic stress damages the function and structure of their still-developing brains. These injuries relate specifically to the prefrontal cortex and academic processes, especially executive function, memory and literacy.
Neurobiology informs us that cognition shuts down; it is physiologically impossible to learn, for the 22% to 45+% of children who are overwhelmed by a state of chronic, or complex trauma. “Equal Access” requires significant accommodations.
The physiological process also leads kids to distorted perceptions of social cues, which alter their social behaviors in response. Eminently logical defenses in the midst of trauma (hyper-vigilance, dissociation) become ingrained habits, and then destructive, once the threat is extinguished, but the defense pattern remains.
Without accommodations leading to equal access, children risk having their traumatic experiences re-triggered and further embedded neurobiologically.
Instead of repair, more damage!
.
Frontline Perspective From the Classroom
Schools could be safe and even restorative. Instead, the childhood trauma crisis disrupts all schools at times. Whether angry, aggressive, violent, or quietly dissociating, trauma-impacted children’s defenses block their own learning and can distract, frustrate and even endanger other children.
At best, trauma-impacted children are invisible in “the data” and analyses (Try asking for ACE-adjusted, test data). At worst the data is outright misleading, especially for our understanding of academic results including “standardized test” results. The results are a confused, meaningless “average”, including epidemic numbers of trauma-impacted students in defensive “survival” mode with muted cognition.
Pivotal decisions such as ESEA revisions are then based on these deceptive data.
Preparing individual “Section 504” plans for individual children does not address system-wide needs and is not a practical option, given the scope: millions of students.
.
A successful education paradigm requires: a) explicit acknowledgement of childhood trauma, b) screening students, c) training teachers and d) creating “safety” across the learning environment.
Screening students can be as simple as using the “ACE score” derived by counselors as part of annual school registration or re-registration. A wide range of other screening measures is available at the National Child Traumatic Stress Network website.
Confronting the learning impacts and the classroom impacts of trauma requires training. The most efficient approach is through teachers, “first responders” in the classroom, who see the children daily. Training must be an on-going requirement to stay current with almost continuous research, to better: 1) deliver“safety”, 2) understand complexity of teaching trauma-impacted children, and 3) respond appropriately, including avoiding re-triggering old trauma.
Other crucial investments towards safety include appropriate class-sizes, with limits on trauma-impacted children per classroom. For example, one teacher alone will struggle to be effective aiding one ‘triggered’ student from among the 10 who have 3+ ACEs, within a classroom of 30 kids, total, who are waiting to be taught. Additionally, dedicated appropriate space for children to de-escalate is needed, as well as on-site counselors; counselors, who build on-going relationships with the children and families in the school community.
.
“We must not look the other way”
Traumatized children need accommodations for equal access to their education.
A common sense revision to ESEA.
The intersection of childhood trauma and our educational system is the most accessible entry-point to this horrific national crisis. Virtually all children in the USA traverse some school every weekday. Innocent children. The semantics are important. They’re not bad, they’re not sick: they are injured, and yet, lawmakers have not acted!
“Childhood trauma” is the key missing, macro factor in education. It has been blurring our interpretation of results for all micro programs.
Meanwhile, we continue pouring billions into education program “buckets” oblivious to the gaping trauma holes in the bottom.
Traumatized children need accommodations for equal access to their education.
.
Now, with the ESEA rewrite, we have a choice to ‘Defend Childhood’, to improve access to education and to bring clarity to results, by explicitly confronting childhood trauma. That, in turn, will lead to more equity in education, and better social and financial productivity for our nation.
.
Action:
Ask your Senators and Representatives to add this crucial factor in their revisions to ESEA.
Key communication points are the “Wide Scope”, the “Deep Impact” and many points in subtitle “Frontline Perspective”.
Click the ‘OpenCongress’ link below to get names of your Congress members. Click on individual name and then find contact information on right side of screen. Email or call them today, or send them a link to this blog. Ask them to acknowledge and fund accommodations in ESEA for trauma-impacted children! More details are outlined under “Frontline Perspective”, above in this blogpost.
https://www.opencongress.org/people/zipcodelookup
Sample note:
Dear ________________________,
Please help millions of trauma-impacted children get “equal access” to their education as part of ESEA.
The wide scope and the deep impact of unaddressed childhood trauma are well documented, including by the Department of Justice, the CDC and the Surgeon General. See “Common Sense” at LucidWitness.com .
A successful education paradigm for trauma-impacted children requires: a) explicit acknowledgement of childhood trauma, b) screening students, c) training teachers and d) creating “safety” (detailed at “Common Sense” at LucidWitness.com) across the learning environment.
Thank you for your support of educational equity.
Sincerely,
